Trusted care from experienced specialist doctors
Personalized, accurate treatment
Holistic care with no side effects
On-demand care, no appointment needed
In-house pharmacy : Convenient Access to Quality Medications


At MCCI Cancer Center, we combine expert homeopathic care with a personalized approach to healing. Our treatments are gentle, effective, and free from side effects—designed to support each patient's unique journey with care and compassion.





Serving Countless Satisfied Patients
Best Homoeopathic
Cancer Hospital
At MCCI Cancer Center, we offer specialized, side-effect-free homeopathic treatments for a wide range of health conditions. Our personalized approach ensures care tailored to each patient’s unique needs.
Treatment support for major cancers including Breast, Lung, Prostate, Colorectal, Skin (Melanoma), Leukemia, Lymphoma, Ovarian, Pancreatic, and Brain Tumors.
Gentle and supportive homeopathic remedies for various heart conditions to improve overall cardiovascular health.
Natural care for Alzheimer’s and other age-related memory conditions to preserve mental clarity and quality of life.
Holistic treatment for diabetes to help regulate sugar levels and reduce complications without side effects.
Homoeopathic solutions for anxiety, depression, insomnia, and other psychological conditions with personalized care.
Specialized support for post-stroke recovery, improving mobility, speech, and cognitive function.
Gentle, individualized support for children and adults with autism to enhance communication, behavior, and quality of life.
Effective homeopathic treatment for asthma and other chronic respiratory conditions, offering lasting relief without side effects.
Get to know the driving force, the visionary leader behind MCCI, whose unwavering dedication and commitment led to the development of solutions for numerous ailments capable of transforming lives.
Dr. A. I. Hidayathullah is a passionate doctor and researcher, driven by a relentless pursuit of innovation in homeopathy. His commitment to finding real treatment solutions for cancer and other chronic diseases has reshaped traditional medical practices, inspiring breakthroughs and new approaches in the field. MCCI represents the realization of his long-envisioned dream of providing proper treatment to all those in need, transforming their lives for the better for-ever.
Through dedication and expertise, he has earned widespread acclaim and recognition, garnering trust and admiration from patients and peers alike. His wealth of experience not only shapes the clinical excellence of our services but also instills a culture of continuous learning and growth within our institution.

We bring a new dimension to homoeopathic care through our specialized divisions, each committed to excellence in treatment, innovation, and community well-being. Together, they reflect our mission to make natural healing more focused, effective, and accessible.

Premium pharmaceutical innovations: Manufacturing premium, research-backed homoeopathic formulations for human healthcare needs

At the Manakkal Center for Cancer and Incurables (MCCI), we have successfully treated numerous cancer patients and complex chronic conditions through our advanced homoeopathic approach.

Delivering cutting-edge veterinary and agricultural homoeopathic solutions to enhance livestock health and crop vitality.

Our Authorised Pharmacy Outlets. Delivering trusted homeopathic and integrative medicines, Manakkal Remedies ensures consistent availability of genuine formulations. As our official pharmacy outlets, they serve as the first point of access for patients seeking quality care and expert guidance in their healing journey.
Skilled. Caring. Committed
Our team of qualified doctors is dedicated to delivering safe, personalized, and effective homeopathic care. With strong clinical knowledge and a patient-first approach, we ensure every individual receives the attention and treatment they deserve.

Dr. Gulshan Rehmani
BHMS |
Reg No 15053

Dr. Aswani N
BHMS | Reg No 13167

Dr. Shabnam KV
BHMS | Reg No 13397

Dr. Hadiya
BHMS | Reg No 13126

Dr. Mahfooz Hassan
BHMS |
Reg No 12076

Dr. Naseef Kuttiyott
BHMS |
Reg No 14948

Dr. AJAY JOSE
BHMS | Reg No 14723

Dr. A.I Hidayathullah
BHMS | Reg No 4916


Every disease is a difficult journey when you have to go through it all alone. We won’t let that happen to you. Let’s get through this together.





Homoeopathy is a natural healing system that works on the idea that a substance causing symptoms in a healthy person can help heal similar symptoms in someone who is unwell — a concept known as “like treats like.” At MCCI, we apply this method by using minute doses of natural ingredients to gently encourage the body’s own healing response.
Unlike conventional treatments that often focus only on relieving visible symptoms, homeopathy looks deeper — aiming to correct the root imbalance that’s causing the illness. This approach is safe, gentle, and well-suited for all age groups, including those managing long-term or complicated health conditions.
Yes, at MCCI, we are committed to offering supportive care for individuals dealing with cancer through a holistic homeopathic approach. Our focus is not only on easing physical symptoms but also on addressing the emotional and mental challenges that come with the illness.
Homoeopathic remedies at MCCI are selected based on the person’s overall constitution — taking into account their physical, emotional, and psychological well-being. This individualized treatment helps in improving comfort, enhancing emotional strength, and supporting the immune system during the course of cancer.
While homeopathy is not a replacement for conventional cancer treatment, many patients find that it plays a valuable role in reducing side effects, improving quality of life, and fostering a sense of balance and hope.
We invite you to explore the heartfelt experiences of those who have walked this path with us — real stories of strength, recovery, and resilience.
At MCCI, we offer homeopathic care for a wide range of health conditions, including thyroid disorders, cancer, infertility, migraines, PCOD, IBS, chronic cough, and fatty liver. Our approach focuses on treating the person as a whole — not just the symptoms — by considering physical, emotional, and mental aspects of health.
Every treatment plan is tailored to the individual, aiming for long-term wellness and balance. Recognized for providing effective homeopathic support, especially in cancer care across Kerala, MCCI is committed to integrating natural healing with modern medical understanding for better outcomes.
Yes, homeopathy is considered safe for people of all ages, including infants, pregnant women, and the elderly. It has no known side effects when prescribed by a qualified homeopath.
The duration varies depending on the individual and the condition being treated. Some experience relief quickly, while chronic conditions may require more time for noticeable improvements.
Homeopathic treatment can be considered at any stage of cancer, from dignosis to post treatment care.


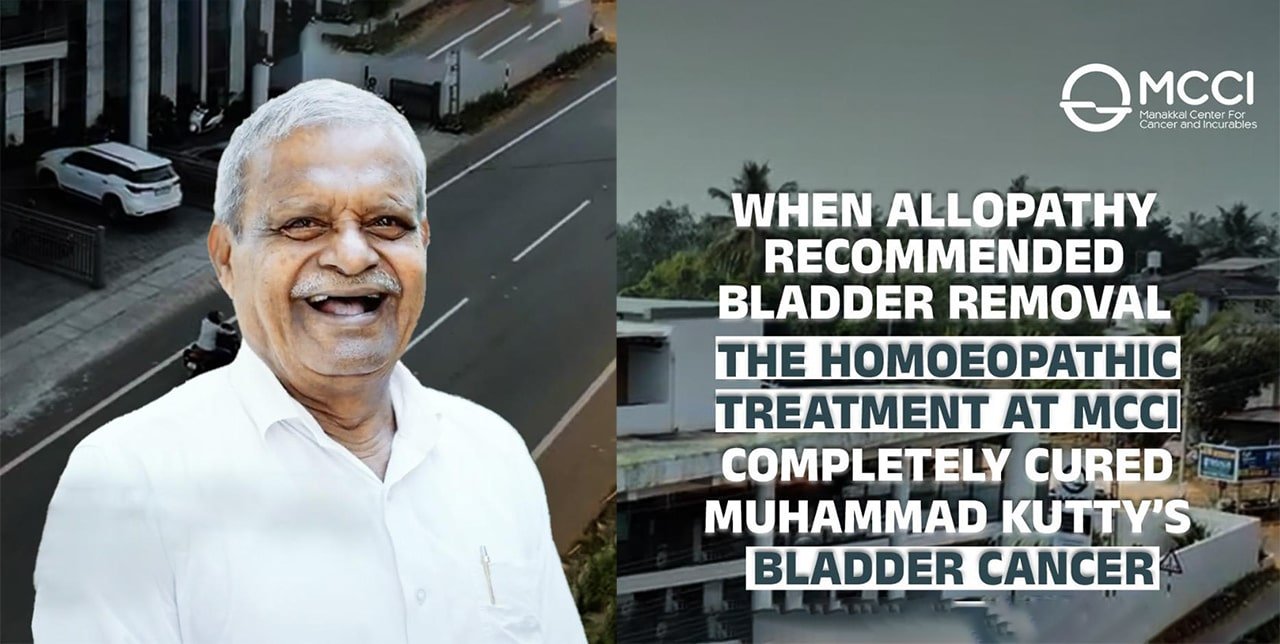
When allopathy recommended bladder removal, I was devastated. But choosing homeopathic treatment at MCCI changed everything. With their care and guidance, my bladder cancer was completely cured—without surgery. I’m forever grateful.

Diagnosed with stage 4 cancer, I was told there was no hope. But under MCCI’s homoeopathic care, I recovered and lived to see my Quran commentary published.

After losing my mother to cancer, I chose homoeopathy at MCCI for my stage 2 lung cancer. With no chemo, radiation, or surgery—just compassionate care—I fully recovered. Today, I’m cancer-free and deeply grateful to Dr. Hidayathullah and the healing power of homoeopathy.





Living with Cancerous Bladder; an Alternate Way Treating Cancer Doctors dee...
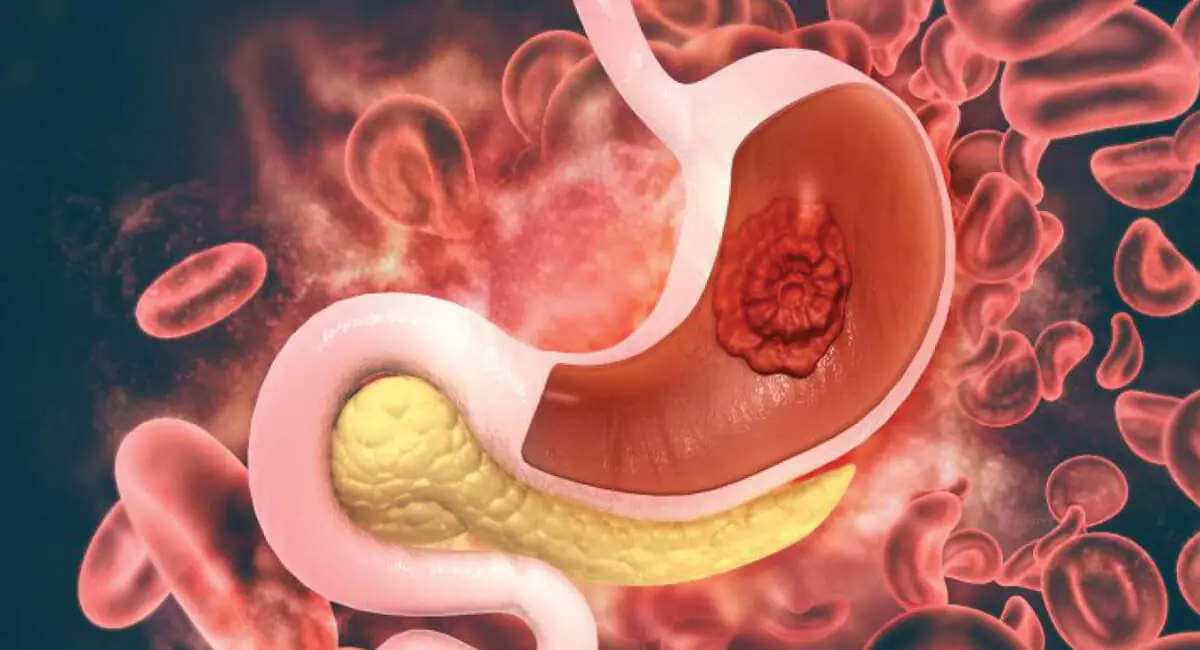
Unregulated cell growth and division in the stomach lining is called stomach cancer or gastric cancer. The stomach is a muscular, ‘J’-shaped organ ...
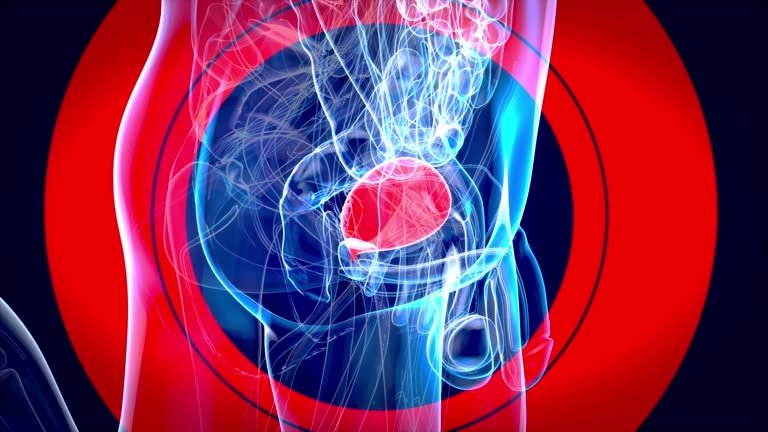
Bladder cancer is a menacing malignancy that originates in the bladder, the organ responsible for storing urine. As one of the most common canc...

